
Th[e] atrocity hierarchy, which one’s nervous system is unfortunately unaware of, is imposed on traumatized people by nontraumatized people, and by themselves. … I’ve never heard it brought up from one traumatized person to belittle another. In the world of the traumatized, the line of sympathy is drawn between those who have PTSD and those who do not.
Regular people, whether they realize it or not, walk around believing, as you cannot make your way in the world without believing, that the universe is holding them.
Well, the people on our side of the line thought, the fuck it does.
Irritable Hearts, p. 126

Content warnings for the middle third of Irritable Hearts (pp 115-201), if you are following along: discussion of rape, suicidal thoughts, and thoughts of self-harm. Realistic descriptions of PTSD symptoms, including intrusion, violent nightmares, and dissociation.
.
.
.
To say that everyone’s PTSD is legitimate is not to say that all PTSD is equivalent. I’m quite clear that I have a mild case of PTSD myself — the equivalent of Stage 1 to J.’s Stage 4.
I’m a little jumpy where J. is constantly hypervigilant. I don’t sleep as well as I used to while J. struggles with life-altering bouts of insomnia and nightmares that shock him awake. I’ve had to work to overcome withdrawal and stay connected to my friends; J. has full blown agoraphobia. I am getting better quicker, and more easily. J.’s healing is a slower, crookeder path, and he has to fight hard for every single step forward.
The question is, then: How do we acknowledge differing degrees of PTSD without forcing people to earn the diagnosis, as we discussed last week? How do we resist applying what McClelland names the “atrocity hierarchy” without saying that all trauma is equal?
How do we acknowledge differing degrees of PTSD without forcing people to earn the diagnosis?
Part of our challenge is that, as we struggle to come to grips with rampant structural and interpersonal violence in the US, we get stuck in a push and pull dance of denial: acknowledge and dismiss, reckon and reject. Add to that the stigma of mental illness more generally and PTSD specifically, and we’re left with squishy sloppy language that can easily confuse or overwhelm.
So let’s spend some time this week seeking clarity. Here are some distinctions that I’ve found useful:
Trauma and PTSD. We often use trauma and PTSD interchangeably, but they’re not the same thing. Trauma is an incident that overwhelms your body and mind’s ability to cope in that moment — anything from natural disaster to divorce to assault to racist microaggressions to a car accident. PTSD is a condition that develops in response to trauma(s) characterized by re-experiencing (flashbacks, nightmares), hyperarousal (excessive vigilance, keyed up startle reflex) and constriction (emotional numbing, addiction, withdrawal, dissociation).
According to the National Institute of Mental Health, about half of US adults will experience at least one traumatic event in their lives — but only a small proportion of them will go on to develop PTSD. Lifetime prevalence of diagnosed PTSD is less than 7%, though women are nearly three times as likely to develop the disease than men.
Activated and Triggered. It’s seems like there is nothing so activating as the word “triggered.” If we ignore or dismiss someone’s claim that they are triggered, we may be minimizing and thus perpetuating very real harm. But if we use triggered to describe every uncomfortable feeling, than we create a false equivalency: If everything is traumatic, nothing is.
That’s why I find the word “activated” so useful. For me, “triggered” means that you have had a bodily response to a sensory input (sound, smell, image, etc.) that brings you back to your trauma as if you are living through it again. It is not an uncomfortable thought or feeling. It’s the precursor to a flashback.
Activated, on the other hand, means you are pushed out of your window of tolerance (more on that below) into a PTSD symptom reaction — panic attack, emotional shut down, hypervigilance. It’s no less real a reaction than being triggered and can also be harmful to mental health. But the cause and the response are different. Activation can arise from emotional, social, or even intellectual discomfort…it is still a process that takes place, at least in part, in the frontal cortex.
It’s seems like there is nothing so activating as the word “triggered.”
There are lots of skills you can use to manage activation in day-to-day life so that you are not pushed down the line into being triggered. You can hopefully walk away from the thing that’s activating you. You can focus on your breathing and ground yourself. You can talk with a friend or therapist.
Being triggered is like getting hijacked by your amygdala. It’s pre-linguistic, a basic survival reflex. Recovering from flashbacks generally starts with trying to bring yourself back to the present moment: engaging your senses to interrupt the unintentional time-travel and arrive back in your body. But mostly, coping with flashbacks and dissociation is preventative. It requires getting to know your triggers and practicing a set of resourcing techniques so you are better able to respond in a crisis. It might take several days, even weeks, to fully recover from flashback or dissociation.
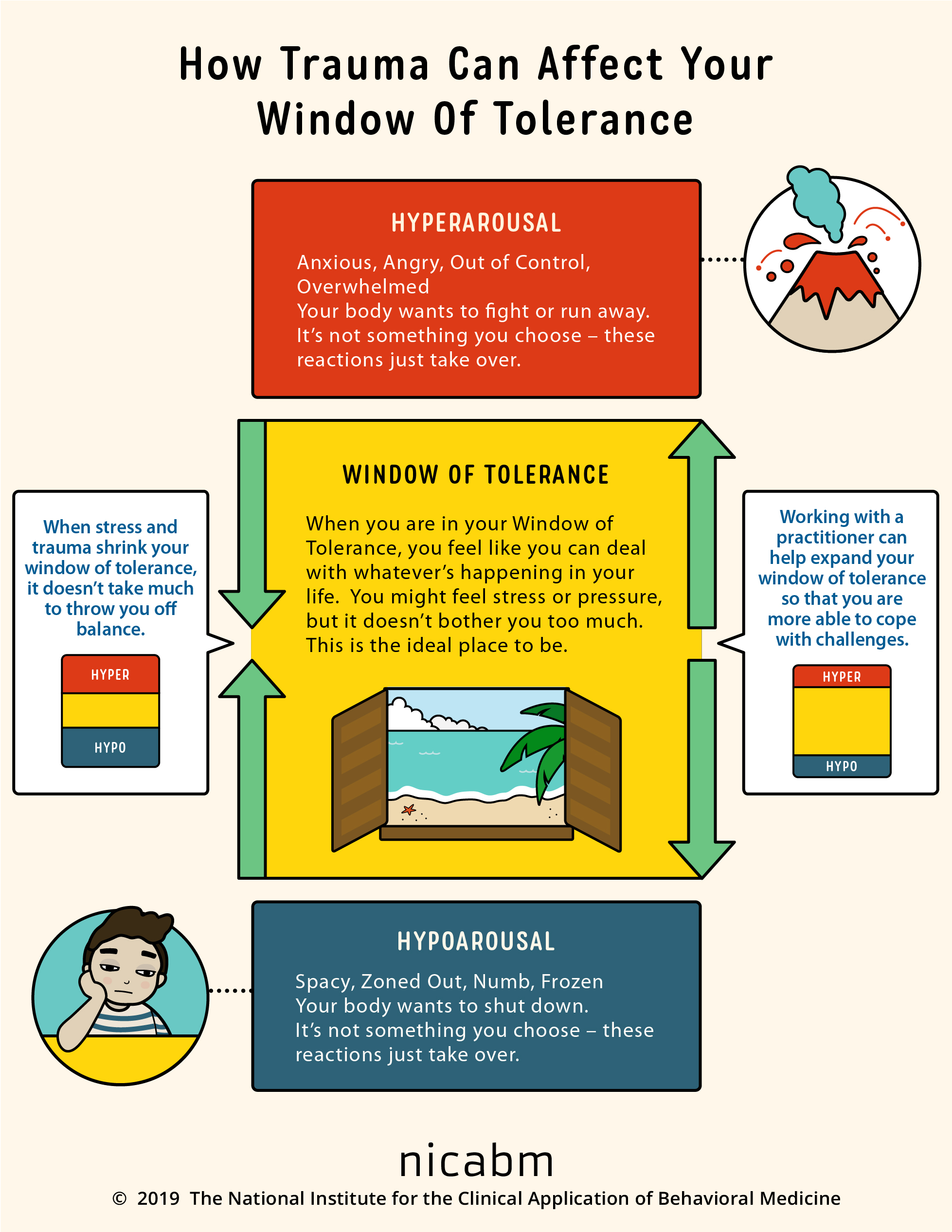
The Window of Tolerance. Finally, I find the concept of the window of tolerance very useful. When we think about PTSD, we most often think only about hyperarousal: flashbacks, panic attacks, hypervigilance, angry outbursts. In other words, trauma turned outwards, with symptoms that are visible and a problem to others.
But equally important are symptoms of hypoarousal: numbness, withdrawal from people or places, addiction. This is trauma turned inwards, and it may give the unfortunate impression that its symptoms are under control. But something like 75 – 85% of people with PTSD have a co-occurring addiction. Dissociation is terrifying. So, the freeze response may be less dramatically visible than fight-flight, but it can certainly cause extraordinary harm.
As NICABM’s graphic shows, trauma shrinks your window of tolerance, and being activated can push you into a hyperaroused or hypoaroused state.
The one beef I have with NICABM’s otherwise useful graphic is the portrayal of being in the window of tolerance as like being on a beach vacation. The aspiration of many therapies for PTSD is to expand the window of tolerance, and that can be incredibly hard, uncomfortable work.
What concepts or language have been useful for you? Share them in the comments below!
.
.
.
* The author of Irritable Hearts now goes by the name Gabriel Mac (@GayyybrielMac, http://gabrielmac.com/) and uses he/him pronouns. When referring to the main character and author of Irritable Hearts, I’ll refer to Mac by the name and gender he was inhabiting at the time of the writing and publication of the book. I don’t want to dead-name him, but many of the points about PTSD and relationships made in the memoir are gender-specific and I want to stay true to those original observations.
Discover more from Virginia Eubanks
Subscribe to get the latest posts sent to your email.

First, I appreciate the use of “activated” in lieu of “triggered” when, at times, the former is more apt. Second, the state of “hypoarousal” is quite familiar to me, unfortunately. And it has been my predominant state for the better part of years.
Finally, for some reason, it hadn’t occurred to me that PTSD can come in a range of severities. I mean, now it is, of course, obvious. I don’t experience the most severe symptoms, myself, for the most part. But for so long, I denied that I had any symptoms at all BECAUSE they weren’t “that severe.” This idea helps me. It also hadn’t occurred to me for a long time that one can heal from PTSD, or improve the symptoms at least. When I realized that, not long ago, it was a big obstacle removed.
I don’t know if any of that makes sense but… thanks for doing this project, V. It has moved me.
Hey Q! I approved this in a rush but didn’t have time to read it closely until now (see the post about abscessed teeth today, alas). Thanks so much for sharing your experience and reflections. Hypoarousal is a nightmare, and unfortunately, if and when you get stuck there, the world seems all too ready to write you off – like “Well, if you’re not freaking out in public, PHEW. Just stay there on your couch, please.”
But YES, PTSD doesn’t have to be from THE WORST TRAUMA IN THE WORLD EVER to be PTSD. That’s what I learned from Irritable Hearts, and it forced me to confront the reality of my own diagnosis when I felt like I had no right to complain because what Jason was going through was so much worse. And YES, PTSD can and does get better. Ain’t none of it easy, but it’s possible. Thanks so much for letting me know that the writing helped you. It means the world to me.